

Hip TEP - Artificial Hip Joint - Hip Prosthesis - Surgery Coxarthrosis - New Hip for Arthritis - Osteoarthritis
Many people know the excruciating groin pain that increasingly restricts freely moving around and thereby decreases the quality of life. Coxarthrosis, the wear of the hip joint, has become a national disease and hip replacements are among the most common surgeries in orthopedics. If a non-surgical treatment no longer leads to a tolerable level of pain, the surgery can often help to end the pain and restore mobility. In recent years implants as well as the surgical techniques have immensely improved: surgery requires only small incisions around the 6 - 7 cm, muscles and bones can be preserved, and post-surgical treatment is relatively short. Surgery promises a quick, pain free condition.
What are the typical symptoms of a hip joint arthrosis / coxarthrosis?
In most cases, the symptoms are groin pain that radiate to the buttocks or from the anterior thigh to the knee. Commonly it is the outside of the hip (greater trochanter) that is affected. For example, tying shoe laces and other activities that require bending down become painful and cumbersome since the hip joint has become stiff. Additionally, walking often becomes painful or is no longer possible. Many patients also suffer from nighttime pain. Interestingly, sometimes knee pain is the only sign of a hip joint disease.
How do I obtain an accurate diagnosis for coxarthrosis/degenerative arthritis of the hip joint?
If a hip osteoarthritis is suspected, a comprehensive clinical examination by an experienced orthopedist is the first step to obtain an accurate diagnosis. Especially in younger patients, the hip pain is often caused by other medical conditions that need to be delineated. In advanced stages of osteoarthritis, typical changes of the joint and in the area of the joint are already noticeable. Further examinations (e.g. ultrasound or magnetic resonance imaging (MRI) is recommended depending on the stage of the osteoarthritis.
In case coxarthrosis is diagnosed, do I need surgery?
Surgical intervention should never be the first step in a therapy (see joint degeneration / osteoarthritis). But if the arthritis has progressed and the non-operative treatment fails, surgery can often eliminate the pain and the walking ability can be significantly improved. When and if a joint replacement is required, is a decision that ultimately you have to make yourself. Decisive in making this decision is less the result of the X-ray, but rather how the osteoarthritis affects the quality of life. Here the range is rather broad: many patients are active despite an advanced osteoarthritis, can perform their daily tasks adequately, and are largely free of pain. Other patients exhibit more severe symptoms that force the patient and the treating physician to consider surgery.
What is the right prosthesis for me?
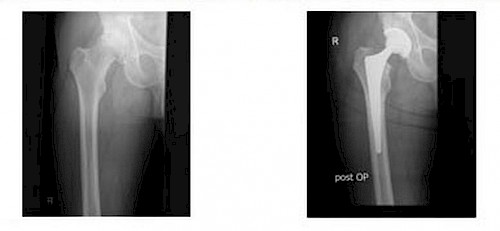
Standard is the shaft prosthesis, which is anchored in the cavity of the existing tubular femur. It is combined with a socket that is fixed in the pelvis. In long-term studies, such a combination has been proven to be the most successful and is therefore the method on which all other methods must be measured. Whether the prosthesis is cemented or attached without cement depends primarily on the individual's bone quality, and it is therefore the first choice for younger patients. By contrast, in softer bone (e.g. in the context of osteoporosis) a cemented prosthesis is the better solution.

Your surgeon knows the selection criteria and will thus choose the best option for you. In addition to the classical forms, other types of prostheses have over time been developed and proven to function successfully – this is very important given the fact that young individuals often experienced a loosening of the prostheses because of their high activity level. This also prompts planning for changes the prosthesis whenever needed As alternative methods are then short stemmed prostheses and surface replacement (cap prostheses) call. The goal of both procedures is to conserve the bone for a firm anchoring of replacement prosthesis. The advantages and disadvantages of the two methods must be discussed with the responsible surgeon. For contact and thus the sliding between prosthesis components at the side of the thigh and pelvis, different materials have proven very durable in terms of their abrasion behavior, biocompatibility, and the durability of the prosthesis. Standard materials today are ceramic, titanium, and highly cross-linked polyethylene.
How is the prostheses implanted?
Most hip prostheses are still implanted today in the two "classic,” for over ten years virtually unchanged way: the lateral and posterior entry to the hip. Both require an incision of about 15 to 25 cm in length, and inevitable require peeling or cutting through muscles. In contrast, the modern, "minimally invasive" access protects the muscles by working through the space between two muscles. The muscle is thus almost immediately after surgery fully functional again without having caused any other injury, which in turn accelerates the rehabilitation after the surgery significantly. The side effect of minimally invasive surgical technique is an incision in the skin averaging 6 to 7 cm. In the KLINIK am RING, all artificial hip joints are being implanted by minimal-invasive surgery already for over ten years.
What are possible complications?
Overall, hip surgery has seen huge progress, so that today, the implantation of a hip prosthesis is a safe procedure. However, it should be clear to anyone who undergoes such a surgery there are residual risks. The surgeon will provide detailed information to the patient prior to deciding on the surgery. An infection, e.g. colonization of the wound or the joint with bacteria is a serious, though extremely rare complication. An infection may lead to one or more subsequent operations. To prevent infection, the surgeon and his or her team will be working under sterile conditions in the operating room and administer preventative antibiotics. Thrombosis is a blood clot in a blood vessel. Preventive blood-thinning medications and standard compression stockings are therefore required for the operation. One problem might be that the length of the operated leg changes because of the insertion of the prosthesis. Generally, the leg that has been affected by osteoarthritis is a little shorter, so that the difference in length can easily be balanced. However, a difference in the length of the legs, can also - of course, very rarely – result directly from the surgery, which can later be corrected by wearing an appropriate insole. A dislocation, which means a dislocation of the prosthesis, is for the most part effectively prevented by avoiding certain movements. Your physician will explain what you can or cannot do immediately after the surgery.
Post-surgical treatment
The hospital stay is about one week during which physiotherapy starts and the wound healing is checked regularly. Depending on the domestic situation and the patient's needs, rehabilitation can be performed on an inpatient or outpatient basis. A minimally invasive surgery generally allows full weight-bearing on the operated hip immediately after surgery since unlike in a traditional surgical procedures no muscle is cut and accordingly a muscle healing is necessary. 80% of our patients can walk the first steps without crutches two days after surgery. Crutches are recommended, however, until you feel secure with the new joint when walking.
What is the lifetime of a hip prosthesis?
Extensive studies have shown that about 95% of the prostheses are still in use after 10 years without a changing operation. After 20 years, 70-80% of the prosthesis did not have to be replaced. This means that even much longer lifetimes of prosthesis are possible.
What determines a successful long-term outcome of a hip replacement?
Within a few weeks or months after surgery, life with a new hip replacement (TEP) will be the same as it would with a healthy joint: You can dance, work, and participate in sports. However, one should not overstress the newly won freedom of movement and refrain from extreme loads (especially activities that include shock movements, highly stressful motions, heavy lifting). Good sports are walking, hiking, cross country skiing, cycling, swimming and dancing, within limits also running. Other factors that influence the durability of the prosthesis, is the body weight, a surgical procedure that causes little trauma to the patient, and the correct positioning of the implant, in other words the experience of a competent surgeon.
Specialists for Arthrosis/Coxarthrosis
Your specialists for hip joint replacement surgeries at the KLINIK am RING in Cologne have extensive experiences with the treatment of arthrosis of the hip joint. They offer the full range of effective therapies, including the implantation of artificial hip joints. In 2004, they founded the WEST GERMAN KNEE & SHOULDER CENTER. After comprehensive examinations and a careful assessment, you will receive your optimal individualized treatment plan.